
Fluoride has been proven to strengthen tooth enamel against decay. That’s why it’s not only added to toothpaste and other dental products, but also to drinking water — in nearly three-quarters of U.S. water systems.
While research has eased most serious health questions about fluoride, there remains one moderate concern. Too much fluoride over time, especially in infants and young children, could lead to “enamel fluorosis,” an excess of fluoride in the tooth structure that can cause spotting or streaking in the enamel. While often barely noticeable, some cases of fluorosis can produce dark staining and a pitted appearance. Although not a symptom of disease, fluorosis can create a long-term cosmetic concern for the person.
To minimize its occurrence, children under the age of 9 shouldn’t regularly ingest fluoride above of the recommended level of 0.70 ppm (parts per million). In practical terms, you as a parent should monitor two primary sources of fluoride intake: toothpaste and drinking water.
Young children tend to swallow toothpaste rather than spit it out after brushing, which could result in too much fluoride ingestion if the amount is too great. The American Academy of Pediatric Dentistry therefore recommends a small “smear” of toothpaste for children under two, and a pea-sized amount for children up to age six. Brushing should also be limited to no more than two times a day.
Your child or infant could also take in too much fluoride through fluoridated drinking water, especially if you’re using it to mix infant formula. You should first find out the fluoride levels in your local water system by contacting the utility or the health department. If your system is part of the U.S. Centers for Disease Control and Prevention’s (CDC) “My Water’s Fluoride” program, you may be able to access that information on line at //apps.nccd.cdc.gov/MWF/Index.asp.
If the risk for developing fluorosis in your area is high, you can minimize your infant’s intake with a few recommendations: breastfeed rather than use formula; use “ready-to-feed” formula that doesn’t need mixing and contains lower fluoride levels; and use bottled water specifically labeled “de-ionized,” “purified,” “de-mineralized,” or “distilled.”
Fluoride can be a wonderful adjunct to dental care in reducing risk for tooth decay. Keeping an eye on how much fluoride your child takes in can also minimize the chance of future appearance problems.
If you would like more information on the possible effects of fluoride on young children, please contact us or schedule an appointment for a consultation. You can also learn more about this topic by reading the Dear Doctor magazine article “Tooth Development and Infant Formula.”










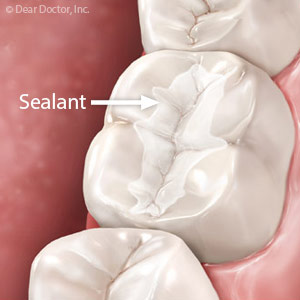
 Issues like cavities can quickly cause the quality of your smile to degrade and cause serious issues if left untreated. You can prevent cavities altogether with a simple dental procedure that takes only minutes. Dental sealants can help protect your teeth from decay and keep them healthy and clean for years. Find out more about dental sealants with Dr. David Doyle at Sunnyside Dentistry for Children in Clackamas, OR.
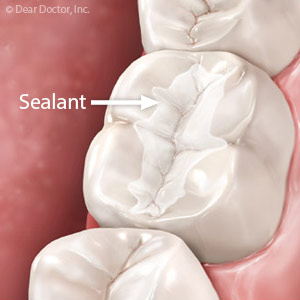
Issues like cavities can quickly cause the quality of your smile to degrade and cause serious issues if left untreated. You can prevent cavities altogether with a simple dental procedure that takes only minutes. Dental sealants can help protect your teeth from decay and keep them healthy and clean for years. Find out more about dental sealants with Dr. David Doyle at Sunnyside Dentistry for Children in Clackamas, OR.




 technique can make children especially susceptible to cavities and tooth decay. And despite the fact that primary (baby) teeth are temporary, they play an important role in your child's development. Dr. David Doyle, a pediatric dentist in Clackamas, OR, recommends scheduling your child's first dental appointment by age one or after 6 to 8 teeth erupt, whichever comes first.
technique can make children especially susceptible to cavities and tooth decay. And despite the fact that primary (baby) teeth are temporary, they play an important role in your child's development. Dr. David Doyle, a pediatric dentist in Clackamas, OR, recommends scheduling your child's first dental appointment by age one or after 6 to 8 teeth erupt, whichever comes first.